Certificate of Need (CON) laws require your doctor or hospital to request and receive a government permission slip before offering you new technology, better facilities, or more treatment options. CON mandates originated under the 1974 federal Health Care Planning Resources and Development Act. According to the Department of Justice (DOJ), a major reason for passing CON was because health care providers at the time were reimbursed on a cost-plus basis. This ignited health care cost inflation, since facilities were paid based on the actual cost of care delivered and comprehensive health plans shielded patients from price sensitivity. Restricting the supply of health care resources under CON was once thought of as a way to cut down on rising health care costs.
In 1987 the federal government repealed its Certificate Of Need mandate, citing CON to be ineffective.
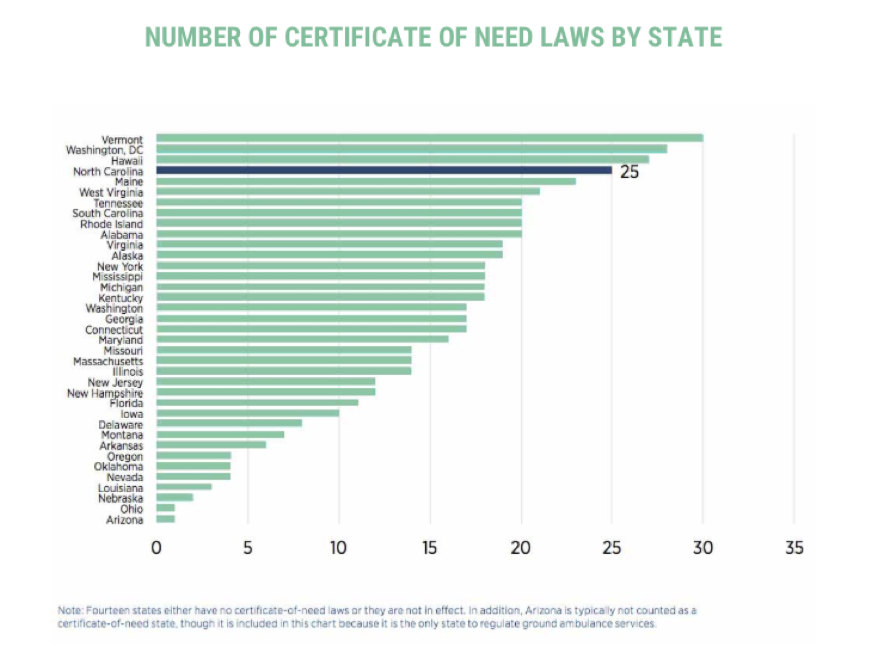
Since then, 16 states have repealed their CON laws. However, North Carolina has one of the most stringent CON laws in the nation. It’s time to restore health care freedom to North Carolinians.
Myth versus Fact
Myth: Hospitals claim that CON laws help them provide more charity care. Limiting competition – especially for lucrative services such as outpatient surgery – allows community hospitals to offset losses from money-losing services with these profits.
Fact: Recent academic research concludes that there is no correlation that CON laws drive higher levels of charity care. Moreover, In North Carolina, there is not a defined percentage of charity care hospitals are required to provide to maintain their non-profit status.
Myth: CON laws are meant to ensure equitable distribution of health care resources and prevent an overinvestment of underused health care resources.
Fact: Statistical studies report that CON correlates with fewer hospital beds, fewer MRI scans, and fewer CT scans, resulting in potential health care access problems for patients. Academic literature suggests that North Carolina CON law results in:
- 12,900 fewer hospital beds
- 49 fewer hospitals offering MRI services
- 67 fewer hospitals offering CT scans
Myth: CON laws are meant to increase access in rural areas and preserve rural health care infrastructure.
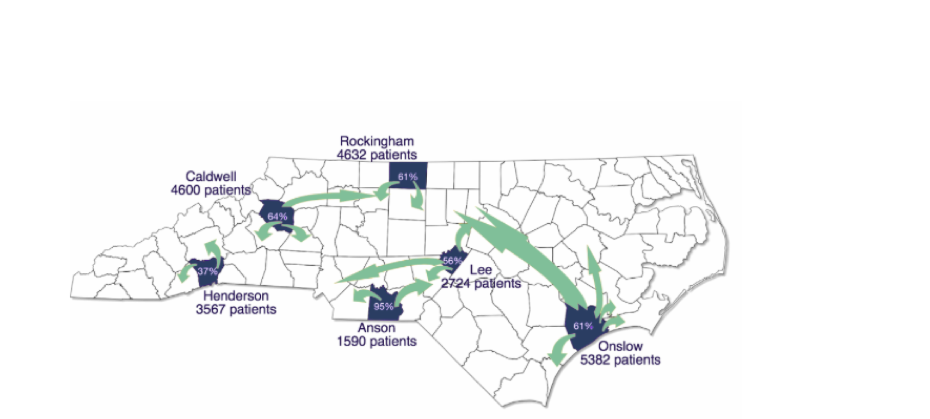
Fact: Compared to non-CON states, North Carolina has 30 percent fewer rural hospitals, and 13 percent fewer rural ambulatory surgery centers (ASCs) per 100,000 rural residents. As a result, rural patients are traveling outside of their communities to obtain outpatient surgery elsewhere because lower-cost, free standing ASCs – just one type of facility regulated under North Carolina’s CON law – are not available in their communities: The map below provides context:
Myth: CON laws control health care costs
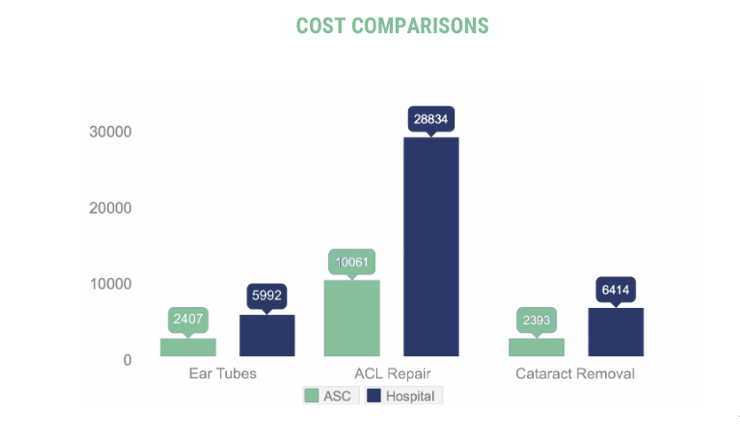
Fact: The federal government concluded 40 years ago that the federal CON mandate failed to control rising health care costs. North Carolina’s CON regulations continue to fail cost control measures. For example, regulatory oversight over ambulatory surgery centers prohibits patients from accessing lower-cost health care options, since these facilities are reimbursed by Medicare on average 45-60% less for the same treatment or procedure performed in a full hospital setting. Today, over 70 percent of the 635,000 annual surgeries in North Carolina are performed in outpatient settings, and 70 percent of these surgeries are conducted in the highest cost hospital systems. Increasing health care supply and availability will make for a more competitive market and help to reduce costs for North Carolinians.
Myth: Deregulating CON will increase health care utilization, driving up health care costs.
Fact: North Carolina implemented CON reform in 2005, in which gastroenterologists were able to bypass CON regulations to perform colonoscopies in their own endoscopy units. Despite utilization of these services increasing by 28 percent over four years, overall Medicare savings amounted to more than $224 million with six years because patients were treated in lower-cost settings.
Resources
http://www.restorehealthcarefreedom.com
https://www.johnlocke.org/acrobat/policyReports/con_laws-macon_no.1.pdf
https://www.mercatus.org/publication/do-certificate-need-laws-increase-indigent-care
http://mercatus.org/sites/default/files/Koopman-Certificate-of-Need-NC-MOP_1.pdf


