Executive Summary
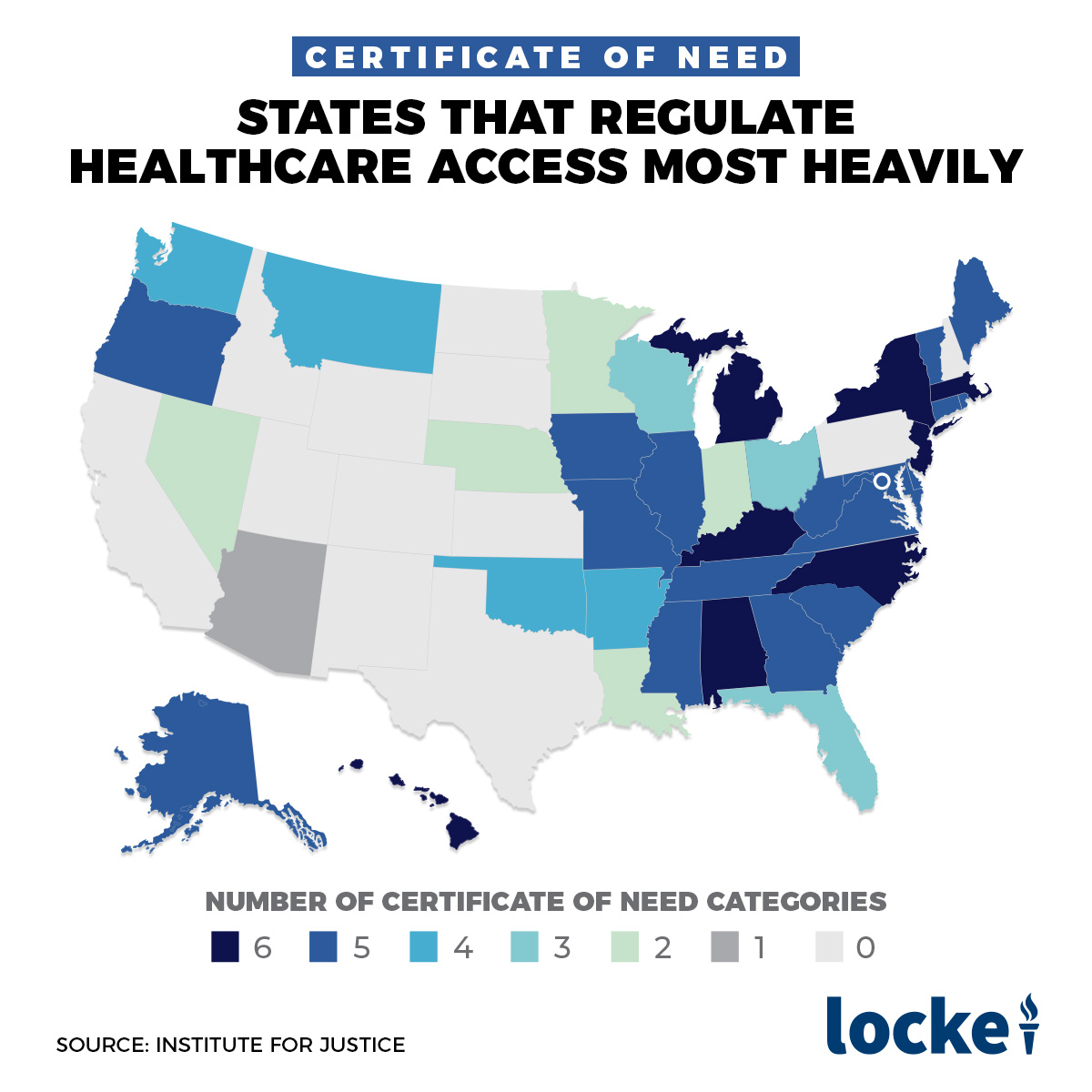
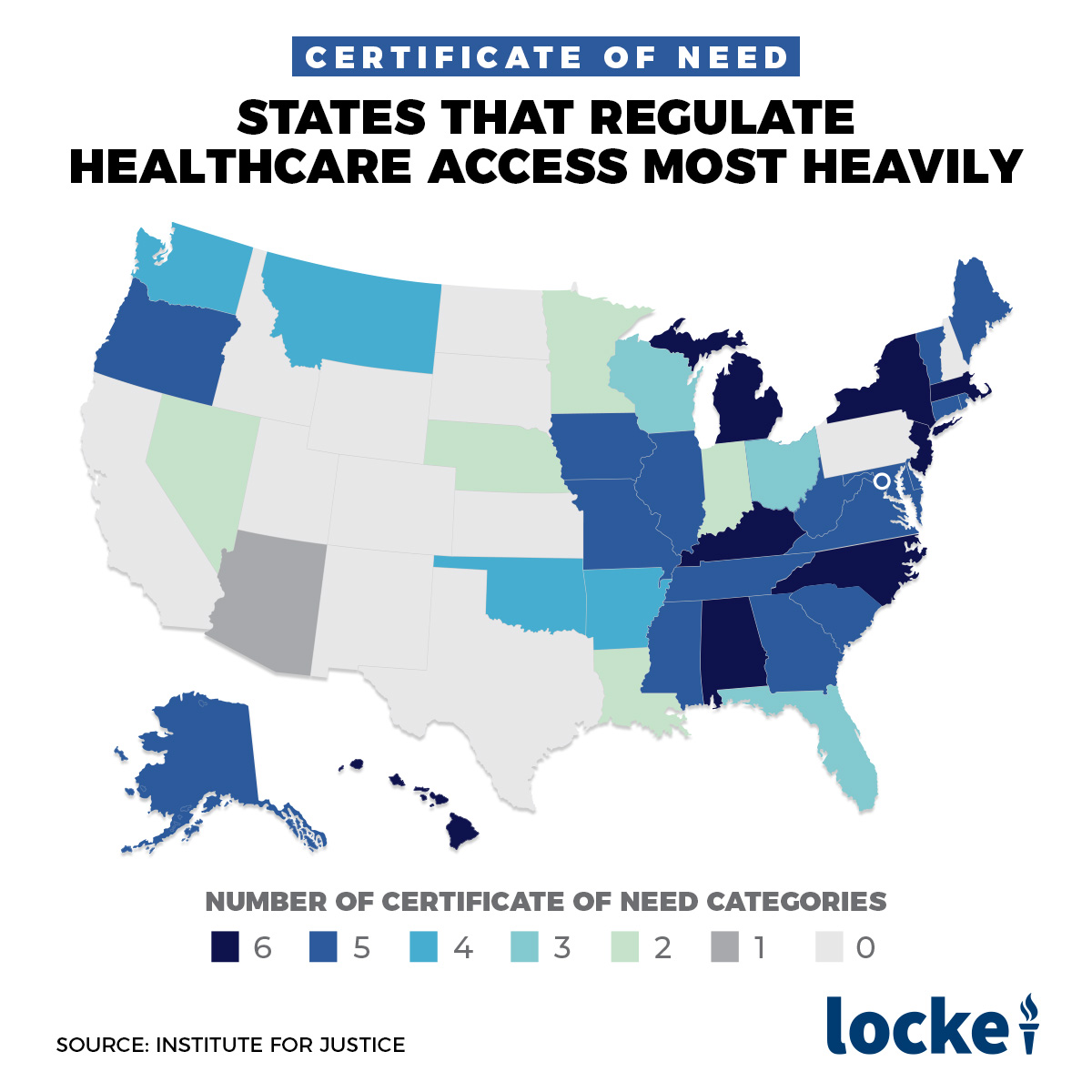
North Carolina is one of 35 states with a Certificate of Need (CON) program, a law requiring health providers to obtain the permission of a state board before opening, expanding, or offering a new type of service. North Carolina’s program is strictest in the Southeast and the third strictest in the country.
In this paper I review the recent academic research on CON, which finds that CON is associated with 30% fewer hospitals per capita, 13% fewer hospital beds, 14% longer emergency room wait times, and 3% higher spending. Reforming or repealing CON is therefore likely to bring more health care facilities, lower health care prices, and better access to care in North Carolina.
These are some of the reasons why organizations as diverse as the Department of Justice, the Federal Trade Commission, the White House Council of Economic Advisors, and the American Medical Association have called for the reform or repeal of CON laws, and why states like New Hampshire and Florida have recently reformed or repealed their CON programs.
Introduction
North Carolina is one of 35 states with a Certificate of Need (CON) program. CON laws require health providers to obtain the permission of a state board before opening, expanding, or offering a new type of service. Most states passed their CON law in response to a 1974 federal mandate1, though 15 states have repealed their laws since the federal requirement was dropped in the 1980s. According to North Carolina’s Certificate of Need program, “The fundamental premise of the CON law is that increasing health care costs may be controlled by governmental restrictions on the unnecessary duplication of medical facilities.”2 In this paper I review the academic research on CON, which shows that if anything CON leads to higher costs, along with less access to care.
This research is part of what led to a dramatic change in the federal government’s approach, from threatening to withhold Medicare funds to states without CON in the 1970’s to asking states to repeal CON today. The Federal Trade Commission and the Department of Justice have released joint statements supporting the repeal of CON laws in several states, including Virginia, Tennessee, and South Carolina3, arguing that CON laws “create barriers to entry and expansion, limit consumer choice, and stifle innovation.” FTC Commissioner Maureen Olhausen went further, calling CON “A Prescription for Higher Costs” in a 2015 article. The White House Council of Economic Advisors questioned the value of CON during both the Obama4 and Trump5 administrations.
The American Medical Association has also argued for repeal, saying that “Certificate of Need (CON) laws have failed to achieve their intended goal of containing costs,” “There is little evidence that CON laws improve access to care,” and “CON programs can impede patient choice,” concluding that “CON laws represent a failed public policy.”
North Carolina in particular has a relatively strict CON program. The American Health Planning Association tracked which of 26 different types of health services, facilities, and equipment were covered by various states through 2016. Their most recent data show that North Carolina required CON for 23 separate types of medical care, making it the third strictest state after Vermont (26) and Hawaii (25). Researchers at the Mercatus Center at George Mason University reached a similar conclusion in 20156. The Institute for Justice compiled a more recent summary of CON laws in the 50 states, noting that “North Carolina is one of eight states to require CONs across all six broad categories — hospital beds, beds outside hospitals, equipment, facilities, services and emergency medical transport.” Their report notes that the CON application process in North Carolina typically takes about 90 days and costs between $5,000 and $50,000 in direct fees. For any potential large project, the most important cost is that the CON application may be rejected entirely, and that the project could then not legally move forward. Making this particularly likely in North Carolina is the fact that “Competitors can intervene in the application process and can offer evidence or argument as to why an application should be denied.”7
Certificate of Need: What Does the Research Say?
Dr. Christopher Conover of Duke University and I conducted a systematic review of the literature on CON laws published before 20108. Surveying the articles that provided original empirical estimates, we found that most research found that CON led to higher spending and worse access to care. Different researchers define “access to care” differently, but for example states that repealed CON were found to have shorter travel times for care9 and smaller racial disparities in care10.
For this report I update my review of the research to include articles published between the year our previous review ended (2010) and 2020. Google Scholar showed 120 publications with “Certificate of Need” in the title between 2011 and 2020. Of these, 55 conducted original empirical research estimating the effect of CON laws on some outcome of interest. I summarize the recent literature on four key outcomes here: health care facilities, health spending, access to care, and the quality of care. Typically, this research compares CON- and non-CON states using regression analysis to control for other differences between states, with some papers using fixed-effects or difference-in-difference analyses that focus on what happens when states pass or repeal CON.
CON and Facilities
The most straightforward and direct effect of CON is that it makes it more expensive, time-consuming, and difficult to open or expand a health care facility and to acquire health care equipment. The academic literature confirms that this generally results in fewer facilities and less equipment in CON states. CON is associated with:
13 percent fewer hospital beds11
26 percent fewer hospitals offering MRI scans and CT scans12
30 percent fewer hospitals per capita13
14 percent fewer ambulatory surgery centers14
49 percent fewer neonatal intensive care beds15
42 percent fewer substance abuse treatment centers16
CON and Spending
Research on how CON affects health care spending found that it leads to 3.1% higher spending overall17 and 13.1% higher spending by patients in less-than-good health18. This higher spending seems to be driven by higher prices more than higher utilization – health care prices are on average 13.8% higher in CON states19, Medicaid spends 60% more per nursing home enrollee in CON states20, and the price of spinal surgery has fallen 11% in non-CON states21.
CON and Access
CON is associated with 14% longer wait times in the emergency department22 and has no effect on the amount of indigent care provided23.
CON and Quality
I focus on mortality here as the clearest and most important measure of quality, though many studies focused on other measures. Two articles studied the effect of CON on all-cause mortality. My own work, published in Health Services Research, found that CON states have 0.5% higher mortality but that the difference was not statistically significant24. A more recent article found that mortality from natural causes is a statistically significant 5 deaths per 100,000 residents higher in CON states, and that when states had high ICU occupancy due to COVID, states that temporarily waived their CON requirements saw 40 fewer COVID deaths per 100,000 residents and 57 fewer natural causes deaths than states that maintained CON25.
One article measured the effect of CON on more specific types of mortality, finding higher mortality rates for patients admitted to the hospital with pneumonia, heart failure, and heart attacks.26
New Research on CON and Treatment for Substance Abuse and Mental Health
My review of the existing research found many articles on how CON affects the provision of physical health care (such as heart surgery and radiation therapy), but none on how it affects the provision of mental health care. To remedy this imbalance and discover how CON affects this important aspect of health care, I conducted two original studies.
In a study27 co-authored with Dr. Eleanor Lewin of Women & Infants Hospital, we measure how CON affects psychiatric hospitals in the 25 states that require CON for psychiatric services (see map). Controlling for a variety of factors, we find that CON is associated with a state having 20% fewer psychiatric hospitals and those hospitals being 5.3 percentage points less likely to accept Medicare. According to 2018 data from the National Mental Health Services Survey, North Carolina had 15 psychiatric hospitals, 12 of which accepted Medicare. Based on our estimates, if North Carolina repealed its CON requirement for psychiatric hospitals, it would be expected to have 18 psychiatric hospitals, of which 15 or 16 would accept Medicare.
In a study28 co-authored with Dr. Thanh Lu of Weill Cornell Medical College and Patrick Vogt of Providence College, we measure how CON affects substance use treatment facilities in the 17 states that require CON for substance abuse treatment. We find that substance use CON has no statistically significant effect on the number of substance use facilities, beds, or clients, and no significant effect on the acceptance of Medicare. However, it reduces the acceptance of private insurance by a statistically significant 1.85%, and the acceptance of Medicaid by a statistically significant 3.49%. According to 2018 data from the National Survey of Substance Abuse Treatment Services, 458 treatment facilities in North Carolina accept cash but only 326 accept private insurance while 349 accept Medicaid. Our estimates suggest that if CON were repealed, an additional 6 treatment facilities would accept private insurance and an additional 12 treatment facilities would accept Medicaid. The result would be more people struggling with substance abuse having access to treatment.
Conclusion: Reform is Possible
The evidence that CON laws are, as the American Medical Association said, “a failed public policy” is overwhelming. But inertia and special interests make CON repeal challenging even when some state policymakers understand the importance of reform. CON leads to costs that are dispersed across the whole population of patients, but its benefits are concentrated among a few incumbent health care providers that use it to keep out new competitors. Each of the handful of firms that benefits from CON benefits a lot, with hospital CEO compensation estimated to be $91,000/yr higher due to CON29, giving them a strong incentive to lobby for the status quo and for favorable rulings from CON boards30. Politicians appreciate these contributions, though they must take care to avoid explicit quid pro quos such as the CON bribery scandal that set in motion the downfall and imprisonment of Illinois governor Rod Blagojevich31.
Meanwhile the costs of CON are dispersed, increasing health spending for a typical patient by 3%32 to 10%33 and doing so in an opaque way – most voters don’t know what CON is. Reform requires farsighted policymakers who are able to look past a handful of complaints from incumbent hospital lobbyists today to a future with more widely available and more affordable health care, new health care providers contributing to their district, and an answer to constituents who ask “what are you doing about health care costs?”
Reform is possible. New Hampshire repealed its entire CON program in 2016 and Florida repealed most of its CON requirements in 2019. COVID and concern about full hospitals led many states34, including North Carolina35, to temporarily waive CON requirements and save lives as a result.36
A recent report from the Mercatus Center provides a variety of options for reforms to CON that stop short of full repeal, while paving the path for a smoother transition to complete repeal. North Carolina’s CON program is by far the strictest in the Southeast, and so a reform that made North Carolina’s program normal would be a major improvement. CON reform in North Carolina would mean that health care providers, rather than state bureaucrats, could decide where new health services are needed. The evidence shows that this would mean more health facilities, better access to care, and lower costs.
Endnotes
1 The National Health Planning and Resource Development Act of 1974; see Conover and Bailey (2020) for a more detailed history
4 Benefits of Competition and Indicators of Market Power
6 Certificate-of-Need Laws: Implications for North Carolina
7 “Conning the Competition: A Nationwide Survey of Certificate of Need Laws”, Institute for Justice
9 Kolstad JT. Essays on information, competition and quality in health care provider markets [PhD [dissertation]]. Cambridge, MA: Harvard University; 2009.
10 Delia D, Cantor JC, Tiedemann A, Huang CS. Effects of regulation and competition on health care disparities: the case of cardiac angiography in New Jersey. J Health Polit Policy Law. 2009;34(1):63–91.
13 Stratmann T, Koopman C. Entry Regulation and Rural Health Care: Certificate-of-Need Laws, Ambulatory Surgical Centers, and Community Hospitals. Mercatus Center working paper (an older article finds a 48 percent decrease- see Eichmann TL, Santerre RE. Do hospital chief executive officers extract rents from Certificate of Need laws? Journal of health care finance. 2011;37(4):1-4.)
15 Lorch SA, Maheshwari P, Even-Shoshan O. The impact of certificate of need programs on neonatal intensive care units. Journal of Perinatology. 2012 Jan;32(1):39-44.
16 Noh S, Brown CH. Factors Associated with the Number of Substance Abuse Nonprofits in the US States: Focusing on Medicaid Expansion, Certificate of Need, and Ownership. Nonprofit Policy Forum 2018 Jun 7 (Vol. 9, No. 2).
17 Bailey J. Can health spending be reined in through supply restraints? An evaluation of certificate-of-need laws. Journal of Public Health. 2019 Dec 1;27(6):755-60.
19 Bailey J, Hamami T, McCorry D. Certificate of need laws and health care prices. Journal of Health Care Finance. 2016 Jul 17;43(4).
20 Rahman M, Galarraga O, Zinn JS, Grabowski DC, Mor V. The impact of certificate-of-need laws on nursing home and home health care expenditures. Medical Care Research and Review. 2016 Feb;73(1):85-105.
21 Ziino C, Bala A, Cheng I. Does ACDF Utilization and Reimbursement Change Based on Certificate of Need Status? Clinical Spine Surgery. 2020 Apr 27;33(3):E92-5.
22 Myers MS, Sheehan KM. The Impact of Certificate of Need Laws on Emergency Department Wait Times. Journal of Private Enterprise. 2020 Mar 1;35(1).
29 Eichmann TL, Santerre RE. Do hospital chief executive officers extract rents from Certificate of Need laws? Journal of health care finance. 2011;37(4):1-4.
31 “She dealt a death blow to Illinois ‘pay to play’”
32 Bailey J. Can health spending be reined in through supply restraints? An evaluation of certificate-of-need laws. Journal of Public Health. 2019 Dec 1;27(6):755-60.
35 https://www.carolinajournal.com/news-article/north-carolina-temporarily-lifts-restrictions-on-hospital-beds/
36 Ghosh S, Roy Choudhury A, Plemmons A. Certificate-of-Need Laws and Healthcare Utilization During COVID-19 Pandemic. Working paper, summarized here



